
RnB Treatment ProtocolTM
This protocol has been developed to help to overcome functional B2 deficiency in Autism Spectrum Disorder, where it is commonly seen that the functional B2 deficiency is reducing the effectiveness of vitamin B12 supplementation. Lack of methylation due to the functional Methyl B12 deficiency, is the major cause of autism.The protocol overcomes the Paradoxical B12 deficiency often seen in the condition (Paradoxical). The use of the protocol is a preparatory step before injection or transdermal application of vitamin B12.The Vitamin B12 protocol, the RnB Treatment protocolTM is the property of B12 Oils Pty Ltd. The protocol is copyright, as such reproduction in whole or in part constitutes an infringement in the Copyright law. Copyright infringement carries serious penalties, including fines of up to US$150,000 and imprisonment..
Riboflavin and B12 treatment
The assumption is that the vitamin B12 deficiency is caused by lack of functional vitamin B2 (FMN and FAD), which has been caused by a lack of vitamin B2 per se, and a possible lack of Iodine, Selenium and/or Molybdenum, all of which are required for the activation of vitamin B2. Such deficiency may come about due to lack of dietary intake of I/Se/Mo or, as is common, lack of these minerals in the local soils. Riboflavin (vitamin B2) is inactive unless it is first activated within the cell. This activation requires three specific steps, which require Iodine, Selenium and Molybdenum. The protocol revolves around a very gradual introduction of Iodine, Selenium and Molybdenum. Introduction is slow as in extreme deficiency simultaneous administration of all three can have strong side effects. Supplementation with vitamin B2 alone will not work, unless there is sufficient Iodine, Selenium and Molybdenum. The protocol is dependent upon identification of deficiencies in the Hair Metals Test Analysis (HMTA). Thus, the protocol addresses those deficiencies that are identified. It should be noted that everyone requires the recommended daily intake of Iodine, Selenium and Molybdenum every day of their life, hence supplementation must be continued after the protocol has been completed, or the diet must be changed to ensure adequate intake of these essential minerals. Functional B2 deficiency can be established by the Organic Acids Test (OAT)(preferrred) or by TSH/T4/T3 assessment. See OATanalysis This can be used to identify deficiency and to interpret the OAT. For further information on OAT go to OAT
NB - You cannot fix functional B12 deficiency unless you fix functional B2 deficiency! Persons using the protocol need to check by OAT that they have been able to fix the functional B2 deficiency or the B12 deficiency cannot be resolved. It the child is still functionally B2 deficient you cannot make progress in resolving the Developmental Delay! If after following the protocol you do not observe a drop in functional B2 deficiency markers, it is important to identify what the problem is.
NNB The over-riding cause of autism is Functional B12 deficiency, which then results in reduced methylation and low energy efficiency. In turn it is functional B2 deficiency that is causing the functional B12 deficiency, which is what is causing the autism, therefore if you do not fix the deficiencies that cause autism you cannot fix the problem. Implicit in the Protocol, though is the need for biologically active vitamin B12 to be present at all time (See Dopamine Paradox), particularly Methyl B12.
NNNB, most people will have normal to high serum B12 BUT it is inactive. see https://b12oils.com/paradoxical.htm It is necessary to displace the inactive B12 with the mixed Adenosyl/Methyl B12 topical oils. This is an essential part of the protocol. In many instances people cannot make the protocol work until they introduce Methyl or Adenosyl/Methyl B12!! This is due to the Dopamine Paradox, in which thyroid function is inhibited in high dopamine levels (see DopamineParadox). It must be noted, that Neurotypical Delay will/can occur in vitamin B12 deficiency alone, and in this case it is reversed just by addition of vitamin B12.
Iron-sulphur protein production. An essential part of energy production in the cell requires the synthesis of iron-sulphur proteins, this can only occur if sufficient Methyl B12 is present, which is another reason for why you MUST include Adenosyl/Methyl or Methyl B12 as part of the protocol
Caution
The protocol assumes that you are low on all of Iodine, Selenium and Molybdenum, which can be assessed by analysis of HMTA and/or thyroid markers. If the person with autism is already sufficient in Iodine, or Selenium or Molybdenum, as judged by these markers, then do not need to necessarily supplement the mineral you are sufficient in. Everyone, regardless, does require at least the Recommended Daily Allowance (RDA) or Recommended Daily Intake (RDI) of Iodine, Selenium and Molybdenum. If you do not get this then the activation of vitamin B2 will be compromised. The ranges listed represent minimum and maximum ranges of daily intake for a person who is replete in Iodine, Selenium and Molybdenum. The protocol also assumes that the person with ASD is not currently supplementing with a multivitamin. Further, if you give the incorrect forms of I/Se/Mo the protocol will not work. There is a schema depicting the whole pathway.
As one parent has said “It is important that parents of children with ASD understand that these kids have been deficient since the womb” and so yes “they may need very high dosages to replete in the co factors”. There is a corollary and that is “As the children start to fix the deficiencies, the demand may go up still further”. There is a caveat, however - The Wolf Chaikoff effect" (See below),
Caution2.
"Ingestion of large quantities of iodine (>1000 ug/day is potentially toxic) causes “downregulation” of the NA/I symporter resulting in decreased thyroid hormone synthesis and secretion of thyroid hormones as a protective effect by the thyroid. This autoregulatory mechanism has been described as the “Wolff Chaikoff effect”." (Prof Cres Eastman - Thyroid Specialist, personal communication; Matthews etal, 2022). Chronic over-consumption of Iodine leads to toxicity on the thyroid resulting in hypothyroidism and goiter (Baker, 2004; Calil-Silveira et al, 2016; Hussein Ael-A, et al 2012; Man et al, 2006; Eng et al, 1999; Uyttersprot et al, 1997). Further, Chloride and Iodide are both anions, and contribute to the osmolarity of serum. Overdosing of Iodide can lead to displacement of Chloride ions and as such it is possible to get the body to retain as much as 10,000 times as much Iodide as normal.
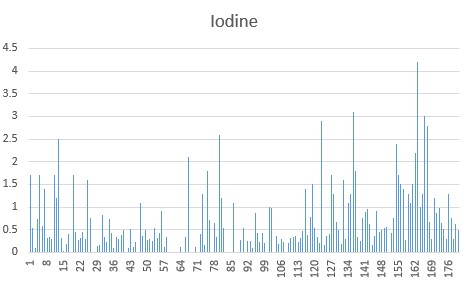
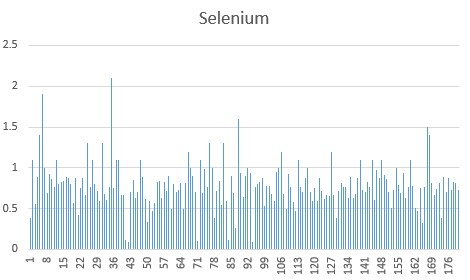
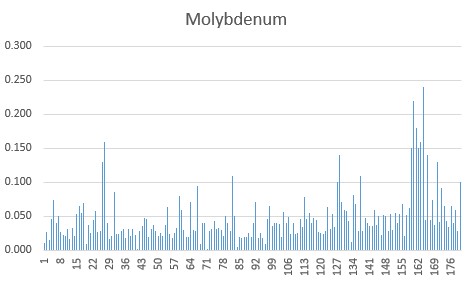
Representative HMTA values of Iodine, Selenium and Molybdenum in children with autism. As can be see the majority are deficient in Iodine (<0.5 ppm), Selenium (<0.7 ppm) and/or Molybdenum (<0.05 ppm)/
First start by introducing Iodine
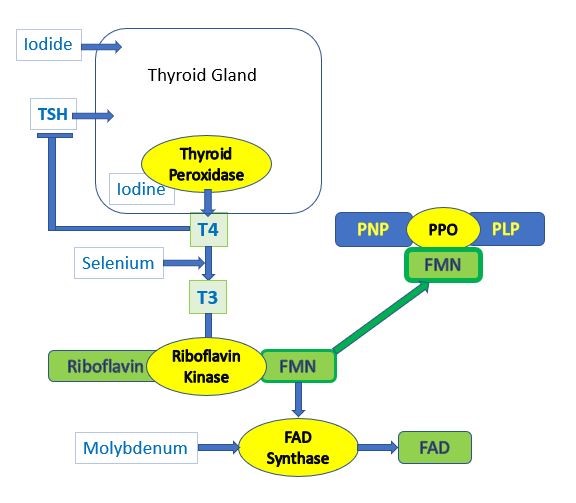
Iodine is at the top of the vitamin B2 activation cascade, as pictured below. (Iodine - I, Selenium - Se, Molybdenum - Mo), For this reason you have to have optimal Iodine levels or the cascade of activation will be compromised.

Iodine build
Start with 50 ug/day for one week and increase to 100 ug/day, week 2. Week 3 and ongoing 150 ug/day. The iodine should be as either the Sodium or Potassium Iodide salt. Iodine does not work, it must be Iodide
Iodide is essential for the production of thyroid hormone (T4)
Natural sources of Iodine are: Seafood, Dairy, Eggs, Grains, and fortified products such as Iodized bread and Iodized salt.
You should avoid goitrogens, such as soy, Cassava, Broccoli, Cauliflower, Cruciferous veggies, and Kale (Goitrogens can affect your iodine levels (iodine-resource.com)_.
Symptoms of over-supplementing with Iodine are generally flu-like symptoms, drowsiness, brain fog following Iodine supplementation, and a drop in TSH below 0.5. RDA for Iodine is 150-300 ug/day (each and every day).
A suitable product is the topically applied Sodium Iodide oil (https://b12oils.com/order.htm ) which can be really titrated up from one drop (~ 74 ug), to 2 drops (150 ug), to 4 drops (300 ug). Topical application avoids interaction of Iodide with food or other supplements
Our data suggests that a suitable target for Iodine can be assessed by monitoring TSH, where a target of between 0.5 and 1.5 should be aimed for. This is in agreement with suggestions made by Kelly (2018) and Cohen and co-workers (2018) and Hanz and co-workers (2020). If your TSH is above 1.5, then you need more Iodine, if it is below 0.5 you may need less Iodine. Avoid using excess Iodide (greater than 600 ug/day). You can assess Iodine sufficiency by urinary output.
Selenium build
After 2 weeks of Iodide supplementation (week 3), continue with the Iodide and add 25 ug/day Selenite and slowly build to 200 ug/day. Start with 25 ug/day for one week and increase to 50 ug/day, week 2. Week 3, 100 ug/day, with week 4 and ongoing 200 ug/day. Adjust doses for children.
Selenite is essential for the conversion of T4 to T3, which is then used to turn on the production of the enzyme Riboflavin kinase which converts riboflavin to FMN. In functional vitamin B12 deficiency, oral selenium will not be taken up from the intestine, so TransdermOIlTm Selenite would be most efficacious.
The RDA for Selenium is 55-200 ug/day, and the aim is to achieve this. In children under 10 aim for 55ug, for adults 200 ug. The selenium should be as the Selenite, or Selenate salt, but should not be Selenomethionine or Selenium chelates, or Selenium amino acids complex, each of which has been shown not to work.
Natural sources of Selenium are: Eggs, Tuna, Shrimp, Beef, Turkey, and wheat from Selenium sufficient soils. Organic foods or gluten-free foods are often low in Selenium as too wheat from selenium depleted soils such as the UK, much of Europe, New Zealand, much of Australia and many States in the USA.
Due to the poor maturation of the gut in many children with autism, topical administration of Selenite is preferred, however, if the material is to be given orally, avoid administering any product with diatomaceous earth, fulvic acid, large dose vitamin C or those with citrate as a preservative, as they can reduce absorption of Selenite (Robinson etal, 1985; Ip, 1986)
Avoid natural source of Calcium, as these bind up the Selenite, thus avoid giving the material in milk. Similarly avoid giving the material in acids, particularly vitamin C and citric acid, as these reduce the Selenite and make it non-available.
A suitable product is the topically applied Sodium Selenite oil (https://b12oils.com/order.htm) which can be really titrated up from one drop (~ 25 ug), to 8 drops (200 ug). Topical application avoids interaction of Selenite with food or other supplements, which is commonly seen with oral products. Further, in prolonged functional B12 deficiency, the gut transporter for many metals is not functional and so oral administration does not work.
At this stage, T3 should start to turn on the production of riboflavin kinase, which will enable conversion of riboflavin to FMN. This, though is only the first step in riboflavin activation.
Molybdenum build
At week 4, continue with the Iodide and Selenite. Start with 50 ug/day Molybdenum (as the Molybdate salt) and gradually increase to at least 200 ug/day. Some adults have been found to need as much as 300 ug/day. The Molybdenum should be sodium or ammonium Molybdate, NOT a Molybdenum chelate or Molybdenum or Molybdate chelate or Molybdenum amino acids complex. Half the doses for children under 10. The RDA for Molybdenum is 100-300 ug/day. Our studies have shown that over 50% of children with autism are Molybdenum deficient. Similarly studies in 2000 showed that 35% of children were Molybdenum deficient and responded to Molybdenum treatment (Waring and Klovrza 2000)
Molybdenum is also essential for the activity of Sulfite oxidase, which inactivates neurotoxic Sulphite. It is also essential for nitrate reductase, and xanthine oxidase.
Natural sources of Molybdenum are lentils, peas, beans, oats, barley, bread, pasta, but only if they are grown in Molybdenum sufficient soils that are basic.
Avoid natural source of Calcium, as these bind up the Molybdate, thus avoid giving the material in milk. Similarly avoid giving the material in acids, particularly vitamin C and citric acid, as these reduce the Molybdate and make it non-available.
A suitable product is the topically applied Sodium Molybdate oil (https://b12oils.com/order.htm ) which can be really titrated up from one drop (~ 50 ug), to 8 drops (400 ug). Topical application avoids interaction of Molybdate with food or other supplements, which is commonly seen with oral products.
NB, Molybdenum build is essential for the activity of FAD synthase (Giancaspero et al, 2015), which is essential for the conversion of FMN to FAD. FAD is a required co-factor for MTHFR and works with FMN for the activity of MTRR. As such FMN and FAD are required for effective cycling of Methyl B12, and hence for methylation. One could argue, that the Molybdenum build is arguably one of the most important steps in the protocol, and as such is as important as Iodide and Selenite.
Vitamin B2 (riboflavin) build
At week 4 you can slowly start to introduce vitamin B2. Start with 2 mg/day for week 4, 5 mg/day for week 5 and 10 mg/day ongoing (after week 6). You must keep going with the Iodine, Selenium and Molybdenum. It is essential that active riboflavin sufficiency is achieved, or the activation of vitamin B12 will not be complete and active B12 deficiency will still be present. There is currently no B2 (riboflavin oil) so you would need to use an oral formulation.
A schematic on what you are trying to achieve/activate is below.
Low dietary vitamin B2, B12, folate and vitamin D have been shown to affect thyroid function, hence these should be introduced as soon as practicable (Krishnamurthy 2021). In addition, diets high in fats require more B2 for processing and this too affects thyroid function (Sayre and Lechleiter, 2012)
Vitamin B12 (Adenosyl/Methyl B12) build
Studies have shown that it is important to have the active forms of vitamin B12, Adenosyl and Methyl B12 present, to displace inactive serum vitamin B12 - even though levels may be very high. Supplementation should start as soon as is practicable. Start with the mixed Adenosyl/Methyl B12 oil mixture (see https://b12oils.com/order.htm ). It may be necessary to start with just a drop of oil, or use a dropper. Apply the oil into an area of clean dry skin and rub it in like a massage oil. If the child/adult can tolerate the drop, then on the following day increase to 2 drops and gradually increase to a whole squirt/dose. NB you cannot get enough vitamin B12 to restock the brain of a child or an adult from any oral supplement, whether it be lozenge, high dose oral or even nasal delivery. Note, the effect of the combined ISeMo/B2/B12 will take time to become apparent. Myelination is a slow process, and so is repair of damage that occurs in prolonged B12 deficiency. NNB, most people will have normal to high serum B12 BUT it is inactive. see https://b12oils.com/paradoxical.htm NNB, Thyroid function is determined by the amount of B2 and B12, as these appear to affect feed-back on the thyroid (Krishnamurthy etal, 2021). Studies have shown some benefit from injections of methyl B12 alone (Hendren etal, 2016). Numerous studies using high dose oral vitamin B12 on a range of conditions, including ASD, AD, IBD, fatigue and depression have shown this route NOT to be suitable for treatment (Scholten etal, 2018; Robson adn Alvares, 2016).
NB: The liver is the major storage organ for vitamin B12, and so if there is B12, dud or not, it can keep supplying B12 to the body, and hence keep serum B12 levels very high. The body, though is very good at keeping B12, so it binds up B12 with two main proteins, one is transcobalamin, which takes B12 into cells (active or inactive) and the other is haptocorrin, which binds both active and inactive B12. Once these two are saturated, you really don’t know how much B12 you have, as all you have is a very elevated serum B12. The haptocorrin-bound material is returned to the liver for storage and a small fraction is secreted into the stomach via the Salivary glands, but if it is inactive, then when B12 is taken up from the gut via Intrinsic factor, the B12 that is taken up is inactive. It then is “passed” to transcobalamin, but as it is inactive it is useless.
The way to get around this problem is to have lots of free active B12 (methyl and adenosyl), which is where the topical TransdermOilTM is so good. It is unlikely that this gets bound by either HC, or TC in serum because both are saturated. What appears to happen is it is secreted into bile and then it competes with B12 that is in food, or which was bound to HC, and released in the stomach, so it is competing with inactive B12. Hence the higher your inactive B12 was in the past, the longer you have to compete out the inactive. It also means that you have to make sure you have a continuous stream of active B12 around.
NEVER USE CYANOCOBALAMIN
Neurotypical Development and the protocol
It must be remembered that neurotypical development is very slow. Neurotypical development involves extensive differentiation of neuronal stem cells and myelination of neurons, particularly in the frontotemporal and Broca's region of the brain. These are all delayed in autism, and require the resolution of the vitamin B2, B12, iron and vitamin D deficiencies to be resolved before development can resume, or proceed in a neurotypical fashion. If these deficiencies are not resolved one cannot expect NT development to proceed. In this regard, if adults who are NT, prolonged vitamin D deficiency can lead to demyelination of nerves, and correction or remyelination of the nerves, and resolution of vitamin B12 deficiency symptoms can take nearly two years.
Classical Signs of Overt B12 deficiency in children and Babies
Fatigue and extreme tiredness
Muscle weakness - hypotonia
Irritability
Poor sleep
Stomach issues - food intolerance
Failure to gain weight
Delays in hitting developmental milestones, such as sitting, crawling, walking, TALKING, potty training.
Lack of imagination and pretend play.
Signs of Adenosyl B12 deficiency
Whilst many of the symptoms of autism can be solely due to Methyl B12 deficiency, there are similar symptoms of AdenosylB12 deficiency (methylmalonic acidemia), including developmental delay, neurological problems, feeding difficulties, vomiting, lethargy and an increased risk of infection. In addition, there can be episodic ketoacidosis, hyperammonaemia, vomiting, seizures, coma and even death. Nearly every child we have data for is both Adenosyl and Methyl B12 deficient, and it is important to treat both deficiencies.
Preliminary signs that the protocol is working
In severe functional B12 deficiency, one of the early signs of deficiency is hypotonia. The hypotonia appears to be due to lack of production of the methylation product creatine. As methylation is restored, creatine production increases and the hypotonia resolves. Further, failure to gain weight is a characteristic of B12 deficiency, and once the metabolism is fixed, the child may start to put on weight, grow, and in some cases there may be an onset of puberty.
There have also been some wonderful success stories, one of the most curious was "Potty training within 3 months".
Side Reactions
The start of methylation can sometimes induce a higher than normal production of Adrenalin, which can cause some odd side-reactions, such as
Increased fatigue, joint or muscle pain, skin rashes, photosensitivity, irritability, paresthesia, dizziness, sleep disturbances, asthenia, muscle cramps, night sweats, hypertension, hypotension, headaches (especially migraines) and swollen glands. Also reported are heavy perspiration, metallic taste in mouth, chills, nausea, bloating, constipation or diarrhoea, low grade fever, heart palpitations, tachycardia, facial palsy, tinnitus, mental confusion, uncoordinated movement, pruritus, bone pain, flu-like syndrome, conjunctivitis and throat swelling"
If the person attempting the protocol has these symptoms during the dose escalation stage of the protocol, go back to the previous dose for a few days before increasing the dose once more. Be aware that children with autism cannot tell you what these symptoms. Further they have no idea of what is causing the symptoms or how to tell you. The most likely symptom is a rise in blood pressure, which may cause them to experience head-aches.
Depending upon what type of deficiency the individual starts with and how deficient they are in Iodine, Selenium and/or Molybdenum, the child may go through symptoms of adrenalin over-production, serotonin withdrawal or dopamine withdrawal. Part of the withdrawal reaction will be due to the down-regulation of serotonin and/or dopamine receptors during the period of vitamin B12 deficiency. See https://b12oils.com/receptor.htm
Hence the child may go through symptoms of too little serotonin, to making lots of serotonin, which cannot be broken down (serotonin over-load), to then suddenly having serotonin deficiency. These effects can be quite precipitous in nature, and come on with only a small increase in functional B2, then B12 sufficiency. Some of the details are outlined in our publication.
Sudden serotonin deficiency can cause symptoms such as inappetance, insomnia, anxiety, depression, headaches, gut cramps, diarrhoea, blood sugar imbalances.
In functional B12 deficiency, the body can over-produce serotonin, and once you start to fix the functional B2/B12 deficiency, levels of serotonin can drop rapidly and the individual can got through a range of symptoms, commensurate with SSRI withdrawal. Symptoms include, but are not limited to
-
Chills
-
Diarrhoea
-
Difficulty walking
-
Dizziness
-
Fatigue
-
Headaches
-
Impaired concentration
-
Insomnia
-
Irritability
-
Light-headedness
-
Nausea/vomiting
-
Paresthesia (burning, prickly, or skin-crawling sensations)
-
Shock-like sensations (sometimes called brain zaps)
-
Vertigo
-
Visual disturbances
-
Vivid dreams
Other reported side-effects include psycho throwing things and breaking them for fun. Running away laughing, increased stimming, increased misbehaviour bubbling and spitting
For this reason, it is important not to go too fast with the protocol.
Dopamine Withdrawal
All people who have functional B12 deficiency have elevated levels of dopamine, and during the process of fixing the functional B12 deficiency, they may suffer symptoms of dopamine withdrawal. Depending upon how much dopamine the person was making and how quickly it the withdrawal, the symptoms can be minor or severe.
Symptoms include
Anxiety, panic attacks, irritability
Depression, hopelessness, and lack of pleasure
Fatigue, exhaustion and difficulty sleeping
Pain and orthostatic hypotension
Difficulty concentrating, cognitive changes, and low motivation,
Funny tasting breath and low libido.
Explanations of the Receptor interaction can be found at https://b12oils.com/receptors.htm
Vitamin D Deficiency
We have found that over 75% of the children with autism are also vitamin D deficient (see https://b12oils.com/vitamind.htm ). Vitamin D works in concert with melatonin (a methylation product, that depends upon active B12) for the maturation of neuronal stem cells. The advent of the sun protection mantra, and the Slip, Slop, Slap campaign, means that a high percentage of the population is now vitamin D deficient. Vitamin D deficiency is a predisposing factor for developmental delay. Several groups are now actively against the cover-up at all costs mantra put out by various Cancer Councils. To this end, levels of vitamin D need to be increased in the children. The effectiveness of oral vitamin D is poor, and what is more the ability of vitamin D to be activated depends upon functional B2/B12 and iron sufficiency.
Vitamin B1 Deficiency
Most children or adults on GFCF diets are vitamin B1 deficient (as too B2/I/Se/Mo and Calcium). Further B2 deficiency begats B1 deficiency. Vitamin B1 should be introduced at around week 6. At the time of introduction, ensure that you have enough active vitamin B2, because vitamin B1 works with FAD in three of the four enzymes that require vitamin B1 as a co-factor.
Folate Deficiency
Early on in the protocol, avoid folate until the B2 and B12 have been optimized. You can introduce folate (either as folic acid, or 5MTHF - 400 ug/day). You can and should try to get folate naturally in the diet by eating leafy green veggies. This will also provide the essential mineral magnesium. Folate is an essential part of the methylation cycle, and introduction of folate will amplify the rate of methylation. Note, Folinic Acid. :In folate-mediated one-carbon metabolism (FOCM), 5-formyltetrahydrofolate (5fTHF), a one-carbon substituted tetrahydrofolate (THF) vitamer, acts as an intracellular storage form of folate and as an inhibitor of the folate-dependent enzymes phosphoribosylaminoimidazolecarboxamide formyltransferase (AICARFT) and serine hydroxymethyltransferase (SHMT). Effectively this would block folate cycling following processing of 5MTHF by methionine synthase, as the product THF could not be processed by SHMT to 5,10-methylene-THF. In addition, in functional B2 deficiency, there is functional B6 deficiency and so SHMT will not work, but neither will MTHFR, as it is dependent upon active B2 (as FAD) and active B3 (as NADH). In functional B2 deficiency, both SHMT and MTHFR will work, but then so too will folic acid.
Biotin Deficiency
Many people with ASD or CFS believe that the condition is due to an allergy to eggs, and so avoid them. In this case they will more than likely be biotin deficient. Supplement with 150 ug/day - or introduce eggs once the protocol has been established. Biotin deficiency, when severe enough will mask Adenosyl B12 deficiency, and reduce MMA levels.
Iron Deficiency
Uptake and processing of iron requires both active B2 and active B12. Iron deficiency is extremely common in ASD. For neurotypically normal development large quantities of iron are required for the process of myelination of the brain and peripheral nervous system. Estimates are 7 mg/day for children 1 to 8 years old. This estimate is of bioavailable iron, NOT of iron in the supplement. It is best to introduce iron containing meats, such as beef or chicken liver, clams, mollusks or mussels or oysters >> beef, lamb goat, deer, bison, sardines turkey, all of which have much higher iron contents than chicken or pork. Non-meat sources of iron are extremely poorly absorbed.
Alternative Protocol
Buy a multivitamin that has all of Iodine (as Iodide 150 ug), Selenium (as Selenite 55-200 ug) and Molybdenum (as Molybdate 100-300 ug). Start with a low dose (around 1/8th of the above) and slowly increase to a full dose over a period of about 4 weeks. It should be noted that you will also be slowly increasing the dose of vitamin B2, along with the I/Se/Mo.
A suitable product is the topically applied Iodide/Selenite/Molybdate oil (https://b12oils.com/order.htm ) which can be really titrated up from one drop per day to 8 drops per day. Eight drops contains a dose suitable for most children of 150 ug Iodide, 55 ug Selenite, and 100 ug Molybdate. Topical application avoids interaction of Iodide, Selenite and Molybdate with food or other supplements, and is much easier to adjust the dose to be administered than most oral supplements. It has the added advantage that it is easy to apply to children. We have not been able to identify one oral supplement that is suitably formulated with Iodide/Selenite/Molybdate.
Gluten-free Products
Most gluten-free products are deficient in Iodine, Selenium and Molybdenum. Further they are not fortified with either folate or vitamin B1. Additionally they often contain high levels of arsenic, lead, and mercury, which is readily seen by increases in values in Hair Metals Test Analysis, Many people who switch to gluten-free products and feel that they gain some benefit have been found to be sensitive to sulphites and nitrites and are actually molybdenum deficient.
Creatine
Over 40% of methylation is involved in the production of creatine, however, persons on a traditional omnivore diet get around 50% of their creatine from food. Food derived creatine is mainly used in supplementing muscle creatine, with brain creatine normally being produced in the brain. Supplementation with creatine, has not generally been effective for replenishing brain creatine (Roschel etal, 2021) however, in extreme deficiency prolonged dosing of 3 gm/day for over a month has shown some benefit.
Factors that can affect the protocol
Any stress that the child faces will affect the level of functional vitamin B2 that the child needs, and so will delay or hinder the ability to achieve functional B2 sufficiency. Examples include, vaccination, child-hood illnesses, such as RSV, colds, flu, foot and mouth, and many such diseases that are rampant in child-care institutions, COVID, COVID vaccination, etc. In addition foods such as goitrogens and those containing cyanoglycosides - Cassava, kale, Boy Choi, broccoli, broccolini, cabbage, soy, rutabago, spinach, etc. High levels of bromide affect Iodide uptake into the thyroid. The most obvious affect is the inability to lower TSH levels with the protocol. Low iron affects the function of thyroid peroxidase and so will affect the formation of T4 in the thyroid. It has also been shown that high levels of fluoride in the drinking water, or in ground water can cause conditions such as Fluorosis, in which TSH levels remain very high, despite Iodide supplementation. It is therefore essential to remove these contaminants before resuming the protocol (Kheradpisheh et al, 2018; Kutlucan etal, 2013).
Medications that interfere with the protocol
It has been found that many of the medications, such as SSRIs, including Risperidone, Tricyclic antidepressants, Monamineoxidase inhibitors, Benzodiazepines, etc affect the success of the protocol and block effective restoration of neurotypical development in children and adults. Until the child/adult has been "weaned" off these drugs, the protocol will not be fully effective. It is important, however, to consult your doctor before you make any such changes in treatments. Side effects of these drugs can be found at
Risperidone Risperidone Side Effects: Common, Severe, Long Term - Drugs.com including : agitation, akathisia, anxiety, constipation, dizziness, drowsiness, dystonia, extrapyramidal reaction, nausea, rhinitis, and weight gain. Other side effects include: abdominal pain, sialorrhea, skin rash, tachycardia, and xeroderma (McCrackenet al 2002; de Araújo et al 2016; Citrome 2017; Maher et al 2012; Ceylan et al 2017; Chaves et al 2013).
SSRIs About Selective Serotonin Reuptake Inhibitors (SSRIs) (healthline.com)
Potentially suitable supplements
It is quite hard to find a suitable multivitamin that has all of Iodine (as Iodide 150 ug), Selenium (as Selenite 55-200 ug) and Molybdenum (as Molybdate 100-300 ug) in the right forms, and many will require additional supplementation with Iodide, Selenite, or Molybdate. As an alternative, B12 Oils has produced a Mixed Iodide/Selenite/Molybdate topical oil containing 150 ug Iodide, 55 ug Sodium Selenite, and 100 ug Sodium Molybdate. Doses are titratable up from one drop until the required dosage for a child is achieved in 8 drops (see https://b12oils.com/order.htm ).
Iodine Supplements
Iodine should be as the sodium or potassium Iodide salts.
https://b12oils.com/order.htm Iodide Topical Oil 8 drops contains 300 ug sodium Iodide
https://shop.bodybio.com/collections/liquid-mineral/products/iodine-9-liquid-mineral-2oz
https://au.iherb.com/pr/Nature-s-Plus-Potassium-Iodide-150-mcg-100-Tablets/42445
https://au.iherb.com/pr/World-Organic-Liquid-Potassium-Iodide-2-fl-oz-59-ml/7775
Selenium Supplements
https://b12oils.com/order.htm Selenite Topical Oil 8 drops contains 200 ug sodium Selenite
https://www.pureformulas.com/selenium-solution-8-fl-oz-236-ml-liquid-by-allergy-research-group.html
https://au.iherb.com/pr/nutricology-selenium-solution-8-fl-oz-236-ml/17257
https://www.chempro.com.au/NUTRITION-CARE-SODIUM-SELENITE-DROPS-50ML
http://www.iherb.com/Eidon-Mineral-Supplements-Selenium-Liquid-Concentrate-2-oz-60-ml/26013
https://www.amazon.com/dp/B0002UIRBM/ref=psdc_3774471_t1_B000IRJOZ2
https://www.amazon.com/gp/product/B00024D52Y/ref=oh_aui_search_detailpage?ie=UTF8&psc=1
https://www.fair-pure.com/en/selen-50g-from-sodium-selenite-vegan
Molybdenum Supplements
NB only sodium and ammonium molybdate supplements work, as Molybdenum is internalized via a molybdate transporter, and so other forms of Molybdenum do not work (Mendel and Bittner, 2006)
https://b12oils.com/order.htm Molybdate Topical Oil 8 drops contains 300 ug Sodium Molybdate
https://www.metabolics.com/sodium-molybdate-pot-of-90-capsules.html
https://www.fair-pure.com/en/molybdenum-150g-120-tablets-molybdate-vegan
https://www.vitacost.com/nutricology-molybdenum-liquid
https://www.epigenetics-international.com/product/molybdenum-100ml
Combination Supplements
https://b12oils.com/order.htm ISeMo topical oil 8 drops contains KI(150 ug), NaSelenate (55 ug) NaMolybdate (100 ug).
Vitamin B2 Supplements
Liquid B2 supplement from Life Solutions - Micro enhanced Vitamin B2 (riboflavin) Vitamin B2 (Riboflavin) – Life Solutions (lifesolutionsnp.com) 50 mg/tablespoon
Multivitamin Supplements
https://www.naturesway.com/Product-Catalog/Alive-Once-Daily-Women-s-50-Ultra-60-Tabs KI(150 ug), NaSelenate (250 ug) NaMolybdate (75 ug).
https://www.biocare.co.uk/methyl-multinutrient KI (200ug), NaSelenite (200 ug), NaMolybdate (200 ug) MeCbl (400 ug)
Side Reactions
The start of methylation can sometimes induce a higher than normal production of Adenalin, which can cause some odd side-reactions, such as
Increased fatigue, joint or muscle pain, skin rashes, photosensitivity, irritability, paresthesia, dizziness, sleep disturbances, asthenia, muscle cramps, night sweats, hypertension, hypotension, headaches (especially migraines) and swollen glands. Also reported are heavy perspiration, metallic taste in mouth, chills, nausea, bloating, constipation or diarrhea, low grade fever, heart palpitations, tachycardia, facial palsy, tinnitus, mental confusion, uncoordinated movement, pruritus, bone pain, flu-like syndrome, conjunctivitis and throat swelling"
If the person attempting the protocol has these symptoms during the dose escalation stage of the protocol, go back to the previous dose for a few days before increasing the dose once more. Be aware that children with autism cannot tell you what these symptoms. Further they have no idea of what is causing the symptoms or how to tell you. The most likely symptom is a rise in blood pressure, which may cause them to experience head-aches.
Follow Up
Once the person or child has been on the vitamin B2/I/Se/Mo supplementation combined with the mixed Adenosyl/Methyl B12 oils for two months, the urinary Organic Acids test should be repeated in order to check that the regime is working. At this time Contact us and we can help determine if the protocol has been effective. You can also check to see if your I/Se/Mo is in range with the hair-metals analysis
Natural food sources of Iodine, Selenium and Molybdenum
|
|
Tolerable Upper limit |
|
Iodine |
Iodine deficiency >50% of population, |
|
150-300 ug/day |
more likely if no dairy. |
|
|
Hypothyroidism with <20 ug/day |
|
|
Seafood, Dairy, eggs, grains |
|
|
AVOID |
|
|
Goitrogens: Soy, cassave , cabbage, Chard, millet, canola |
|
|
broccoli, cauliflower, cruciferous veggies. Cyanoglycosides: cassava, tapioca, sorghum, lima beans, bamboo shoots. |
|
` |
Deficiency of iron or vitamin A |
|
Selenium |
Tolerable Upper limit - 200 ug |
|
55 -200 ug/day |
Tuna, Ham, Shrimp, Beef, |
|
|
Turkey, Chicken, eggs. |
|
|
Grains, depending upon where they come from. |
|
|
Brazil Nuts have selenomethionine, |
|
|
not selenocysteine. |
|
Molybdenum |
Tolerable Upper limit - 2 mg |
|
100 -300 ug/day |
Lentils, peas, beans, oats, |
|
|
Barley, Bread, Pasta, Rice |
NB. Most gluten-free products are deficient in Iodine, Selenium and Molybdenum. Further they are not fortified with either folate or vitamin B1. Additionally they often contain high levels of arsenic, lead, and mercury, which is readily seen by increases in values in Hair Metals Test Analysis
Role of Vitamin B2
More about vitamin B2 and the effect of deficiency can be found at
https://lpi.oregonstate.edu/mic/vitamins/riboflavin#deficiency-risk-factors
Iron Supplements
The most readily absorbed form of iron is heme iron, from sources such beef, goat, lamb, squid, octopus, mussels, oysters and clams etc. Non-heme iron, such as the iron in quoted vegetables such as soy, lectins, spinach, etc are very poorly absorbed and have not been found to significantly raise serum ferritin levels.
Potential supplements
Ortho Iron (Iron-ferric pyrophasphate/lactoferrin (30 mg) lactoferrin (100 mg), Copper (0.9 mg) https://au.iherb.com/pr/advanced-orthomolecular-research-aor-ortho-iron-60-vegetarian-capsules/73593
ProFerrin ES90 10.5 mg Heme iron https://proferrin.com/international-distribution
General Supplements
Supplements containing Iodide, Selenite, and Molybdate are rather hard to find. Some are listed below:
https://au.iherb.com/pr/Nature-s-Way-Alive-Once-Daily-Women-s-Ultra-Potency-Multi-Vitamin-60-Tablets/39614 KI 150 ug, NaSelenate 250 ug, NaMolybdate 75 ug.
https://www.seroyal.com/trace-mineral-comple-cws.html KI 50 ug, NaSelenate 50 ug, NaMolybdate 50 ug.
https://www.biocare.co.uk/methyl-multinutrient KI (200ug), NaSelenite (200 ug), NaMolybdate (200 ug) MeCbl (400 ug)
https://www.awakennutrition.com/supplement-facts/ KI(100 ug) NaSelenite (50 ug), NaMolybdate (100 ug) MeCbl (1000 ug).
NB, Oral MeCbl in high doses is inactivated in the stomach, so although it may be present in a supplement, its utility in any oral supplement is questionable.
Supplements that may not work due to Calcium and Magnesium content
https://au.iherb.com/pr/Nature-s-Way-Alive-Once-Daily-Women-s-Ultra-Potency-Multi-Vitamin-60-Tablets/39614 KI 150 ug, NaSelenate 250 ug, NaMolybdate 75 ug.
Magnesium 100 mg, Cacium 195 mghttps://www.biocare.co.uk/methyl-multinutrient KI (200ug), NaSelenite (200 ug), NaMolybdate (200 ug) MeCbl (400 ug) Magnesium (60 mg)
https://www.naturesway.com/Product-Catalog/Alive-Once-Daily-Men-s-Ultra-60-Tabs KI 150 ug, NaSelenate 250 ug, NaMolybdate 75 ug. CN Cbl 100ug Calcium 130 mg
https://www.awakennutrition.com/supplement-facts/ KI(100 ug) NaSelenite (50 ug), NaMolybdate (100 ug) MeCbl (1000 ug).
Magnesium (200 mg)Supplements that may not work due to Calcium content
https://au.iherb.com/pr/Nature-s-Way-Alive-Once-Daily-Women-s-Ultra-Potency-Multi-Vitamin-60-Tablets/39614 KI 150 ug, NaSelenate 250 ug, NaMolybdate 75 ug.
Calcium 195 mghttps://www.naturesway.com/Product-Catalog/Alive-Once-Daily-Men-s-Ultra-60-Tabs KI 150 ug, NaSelenate 250 ug, NaMolybdate 75 ug. CN Cbl 100ug Calcium 130 mg
Bayer OneADay https://www.oneada.ca/ Contains Selenite, Molybdate, but also Calcium and vitamin C.
Simple Spectrum Supplement Simple Spectrum Supplement
Supplements that may not work due to Citric Acid content
Nutrisorb® Liquid Selenium 15ml | BioCare Sodium Selenite, BUT, citric acid is the preservative
https://www.biocare.co.uk/nutrisorbr-molybdenum-15ml Sodium Molybdate, BUT, citric acid as the preservative.
Supplements that may not work due to Calcium and Phosphate content
Seeking Health B minus - https://www.seekinghealth.com/products/b-minus-100-capsules Contains Riboflavin-5-phosphate, Pyridoxal-5-phosphate and Calcium pantothenate. The calcium theoretically would dissociate from the pantothenate and then form insoluble complexes with the phosphates on R5P and P5P
https://www.fair-pure.com/en/selen-50g-from-sodium-selenite-vegan "Ingredients: bulking agent microcrystalline cellulose, calcium salts of orthophosphoric acid, sodium selenite"
Supplements that have been shown NOT to work
https://www.bioticsresearch.com/node/1526
Genestra Liquid Iodine
https://www.seekinghealth.com/products/molybdenum-90-capsules
https://www.allergyresearchgroup.com/liquid-molybdenum-1-fl.-oz.-30-ml
https://shop.bodybio.com/collections/liquid-minerals/products/molybdenum-7-liquid-mineral-2oz
Nutrisorb® Liquid Selenium 15ml | BioCare Sodium Selenite, BUT, citric acid is the preservative
https://www.biocare.co.uk/nutrisorbr-molybdenum-15ml Sodium Molybdate, BUT, citric acid as the preservative.
Liquid Iodine Supplement (Nutrisorb®) | 15ml | BioCare Citric Acid is the preservative.
References
Mendel and Bittner, 2005 https://www.sciencedirect.com/science/article/pii/S0167488906001017
McCrackenet al Risperidone in children with autism and serious behavioral problems N Engl J Med 2002 Aug 1;347(5):314-21.
Krishnamurthy HK, Reddy S, Jayaraman V, Krishna K, Song Q, Rajasekaran KE, Wang T, Bei K, Rajasekaran JJ. Effect of Micronutrients on Thyroid Parameters. J Thyroid Res. 2021 Sep 28;2021:1865483. doi: 10.1155/2021/1865483. PMID: 35140907; PMCID: PMC8820928.
Baker DH. Iodine toxicity and its amelioration. Exp Biol Med (Maywood). 2004 Jun;229(6):473-8. doi: 10.1177/153537020422900604. PMID: 15169965.
Calil-Silveira J, Serrano-Nascimento C, Laconca RC, Schmiedecke L, Salgueiro RB, Kondo AK, Nunes MT. Underlying Mechanisms of Pituitary-Thyroid Axis Function Disruption by Chronic Iodine Excess in Rats. Thyroid. 2016 Oct;26(10):1488-1498. doi: 10.1089/thy.2015.0338. Epub 2016 Sep 14. PMID: 27461375.
Hussein Ael-A, Abbas AM, El Wakil GA, Elsamanoudy AZ, El Aziz AA. Effect of chronic excess iodine intake on thyroid function and oxidative stress in hypothyroid rats. Can J Physiol Pharmacol. 2012 May;90(5):617-25. doi: 10.1139/y2012-046. Epub 2012 May 2. PMID: 22550940.
Man N, Guan HX, Shan ZY, Li YS, Fan CL, Guo XJ, Chen W, Tong YJ, Chong W, Mao JY, Teng WP. [Long-term effects of high iodine intake: inhibition of thyroid iodine uptake and organification in Wistar rats]. Zhonghua Yi Xue Za Zhi. 2006 Dec 26;86(48):3420-4. Chinese. PMID: 17313856.
Eng PH, Cardona GR, Fang SL, Previti M, Alex S, Carrasco N, Chin WW, Braverman LE. Escape from the acute Wolff-Chaikoff effect is associated with a decrease in thyroid sodium/iodide symporter messenger ribonucleic acid and protein. Endocrinology. 1999 Aug;140(8):3404-10. doi: 10.1210/endo.140.8.6893. PMID: 10433193.
Uyttersprot N, Pelgrims N, Carrasco N, Gervy C, Maenhaut C, Dumont JE, Miot F. Moderate doses of iodide in vivo inhibit cell proliferation and the expression of thyroperoxidase and Na+/I- symporter mRNAs in dog thyroid. Mol Cell Endocrinol. 1997 Aug 8;131(2):195-203. doi: 10.1016/s0303-7207(97)00108-1. PMID: 9296378.
Mathews DM, Peart JM, Sim RG, Johnson NP, O'Sullivan S, Derraik JGB, Hofman PL. The SELFI Study: Iodine Excess and Thyroid Dysfunction in Women Undergoing Oil-Soluble Contrast Hysterosalpingography. J Clin Endocrinol Metab. 2022 Nov 25;107(12):3252-3260. doi: 10.1210/clinem/dgac546. PMID: 36124847; PMCID: PMC9693785.
Scholten AM, Vermeulen E, Dhonukshe-Rutten RAM, Verhagen T, Visscher A, Olivier A, Timmer L, Witteman BJM. Surplus vitamin B12 use does not reduce fatigue in patients with Irritable Bowel Syndrome or inflammatory bowel disease: A randomized double-blind placebo-controlled trial. Clin Nutr ESPEN. 2018 Feb;23:48-53. doi: 10.1016/j.clnesp.2017.10.004. Epub 2017 Nov 2. PMID: 29460813.
de Araújo et al Quality of Life and Hormonal, Biochemical, and Anthropometric Profile Between Olanzapine and Risperidone Users Psychiatr Q 2016 Jun;87(2):293-304.
Citrome L Activating and Sedating Adverse Effects of Second-Generation Antipsychotics in the Treatment of Schizophrenia and Major Depressive Disorder: Absolute Risk Increase and Number Needed to Harm J Clin Psychopharmacol 2017 Apr;37(2):138-147.
Robson, R, and Alvares, D (2016) The difficulties with vitamin B12. Practical Neurology, 16, 308-11
Maher et al Summary of the comparative effectiveness review on off-label use of atypical antipsychotics J Manag Care Pharm 2012 Jun;18(5 Suppl B):S1-20.
Krishnamurthy HK, Reddy S, Jayaraman V, Krishna K, Song Q, Rajasekaran KE, Wang T, Bei K, Rajasekaran JJ. Effect of Micronutrients on Thyroid Parameters. J Thyroid Res. 2021 Sep 28;2021:1865483. doi: 10.1155/2021/1865483. PMID: 35140907; PMCID: PMC8820928.
Sayre NL, Lechleiter JD. Fatty acid metabolism and thyroid hormones. Curr Trends Endocinol. 2012 Jan 1;6:65-76. PMID: 24436572; PMCID: PMC3891511.
Giancaspero TA, Galluccio M, Miccolis A, Leone P, Eberini I, Iametti S, Indiveri C, Barile M. Human FAD synthase is a bi-functional enzyme with a FAD hydrolase activity in the molybdopterin binding domain. Biochem Biophys Res Commun. 2015 Sep 25;465(3):443-9. doi: 10.1016/j.bbrc.2015.08.035. Epub 2015 Aug 12. PMID: 26277395.
Ceylan et al Effectiveness, Adverse Effects and Drug Compliance of Long-Acting Injectable Risperidone in Children and Adolescents Clin Drug Investig . 2017 Oct;37(10):947-956.
Chaves et al Quality of life and adverse effects of olanzapine versus risperidone therapy in patients with schizophrenia Psychiatr Q. 2013 Mar;84(1):125-35.
Kheradpisheh et al. Impact of drinking water fluoride on human thyroid hormones: A case-control study. Scientific Reports 9 (https://www.nature.com/articles/s41598-018-20696-4
Kutlucan etal The investigation of fluorosis on thyroid volume in school-age children. Med Glas (Zenica) 2013 fe;10(1):93-8 PMID:23348169 https://pubmed.ncbi.nlm.nih.gove/2348169/
Hendren RL, James SJ, Widjaja F, Lawton B, Rosenblatt A, Bent S. Randomized, Placebo-Controlled Trial of Methyl B12 for Children with Autism. J Child Adolesc Psychopharmacol. 2016 Nov;26(9):774-783. doi: 10.1089/cap.2015.0159. Epub 2016 Feb 18. PMID: 26889605.
Roschel etal, 2021 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7916590/pdf/nutrients-13-00586.pdf
Waring RH, Klovrza LV. Sulphur metabolism in autism. Journal of Nutritional & Environmental Medicine. 2000;10:25–32. doi: 10.1080/13590840050000861.
Copyright © 2018 B12 Oils. All Rights Reserved.
Reproduction in whole or in part in any form or medium without express written
permission is prohibited