
Vitamin B12 Deficiency, Receptor Regulation and Depression
-
Deficiency of Vitamin B12 greatly reduces the ability to make adrenalin from the precursors dopamine and nor-adrenalin
-
Deficiency of Vitamin B12 greatly reduces the ability to make melatonin from the precursor serotonin
-
Prolonged deficiency of vitamin B12 eventually results in over-production of dopamine and serotonin
-
Over-production of dopamine and serotonin leads to receptor down-regulation and DEPRESSION and/or ANXIETY
-
Subsequent correction of vitamin B12 depression leads to a rapid drop in dopamine and serotonin and a sudden production of adrenalin and melatonin
-
Symptoms of adrenalin over-production are common
-
Greater depression and/or anxiety can ensue
Vitamin B12 and Production of Adrenalin
Production of Adrenalin/epinephrine is critically dependent upon active methyl-Co(III)B12. The last step in the production of adrenalin is the methylation of nor-adrenalin to produce methyl-nor-adrenalin or adrenalin by the enzyme Norepinephrine-N-methyl-transferase..
Nor-Adrenalin + SAMe => Adrenalin + SAH
In vitamin B12 deficiency, more specifically in methyl B12 deficiency, the levels of SAMe are reduced and hence the levels of Adrenalin are reduced.
In an attempt to overcome this deficiency, the body tries to make more Adrenalin by over-producing the precursor molecules Dopamine and Nor-Adrenalin, whose levels can increase 10 to 20 to even thirty-fold, as judged by their break-down products HVA and VMA (see below).
Vitamin B12 and Production of Melatonin
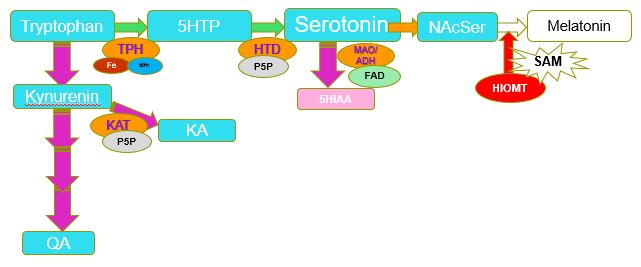
Production of melatonin is also dependent upon methyl-Co(III)B12, following a series of reactions. First the cell takes up tryptophan which is converted to serotonin, which is subsequently acetylated and N-acetyl-serotonin is then methylated by Hydroxyindole-O-methyltransferas to form melatonin.
N-Acetyl-serotonin + SAMe => Melatonin + SAH.
In methyl B12 deficiency, the levels of SAMe are reduced and hence the levels of melatonin are greatly reduced. The body responds by over-importing tryptophan into the cell and by increasing the production of serotonin, and levels of 5HIAA (the serotonin break-down product) can reach levels that are 20 to even 200 times normal levels, whilst QA levels (the breakdown product of tryptophan) can be 10 to 30-fold higher than normal.
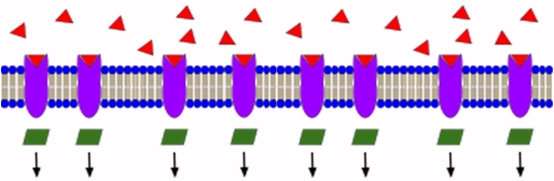
Vitamin B12 Deficiency and Down-regulation of Dopamine and Serotonin Receptors
In most neurotransmitter receptor interactions, control of response to a "normal" amount of neurotransmitter production is finely tuned so that there is a good balance between the amount of ligand (neurotransmitter) and the numbers of receptors so the cell receives a good response signal.
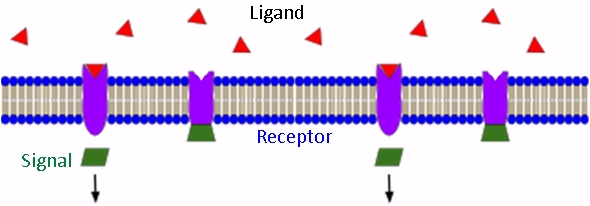
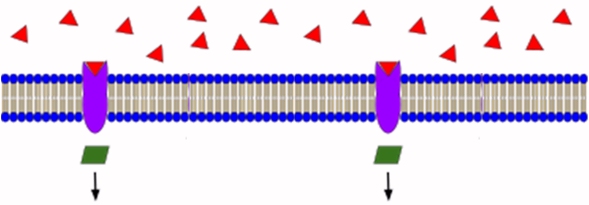
If too much ligand is produced the cell can modify the amount of signal by turning down the production of the receptors a process called receptor-down-regulation. In vitamin B12 deficiency, there is an over-production of both serotonin and dopamine and so one would expect that the number of receptors that can respond to stimulus is gradually reduced. It is reduced too far, then there will be too few receptors to generate a good response and so it will "appear" as if there is no dopamine or serotonin because there is no response. At this stage the person could experience depression.
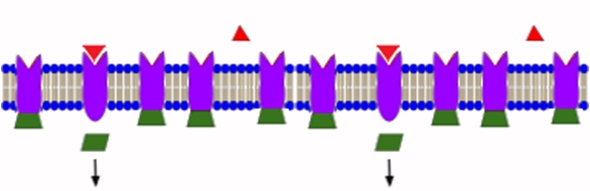
Accompanying the down-regulation of dopamine and serotonin receptors the body can respond to the lower amount of adrenalin and melatonin by turning up the production of adrenalin and melatonin receptors in a process called up-regulation. For a while this will mean that the person does not appear to be B12 deficient, but eventually as levels drop far enough the person will experience adrenal fatigue and symptoms of melatonin deficiency, such as an inability to sleep.
If the person with the B12 deficiency suddenly increases the amount of Methyl B12 levels, serious problems can result. First, the amount of dopamine and serotonin produced will suddenly drop and so now the person, who has already down-regulated receptor production will suddenly have too few receptors to respond to the greatly reduced amount of dopamine and serotonin and so may experience extreme depression, in a similar fashion to any drug addict coming off medication.
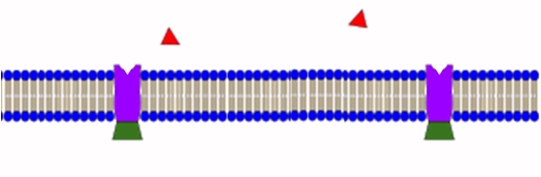
Second, the sudden production of large amounts of adrenalin can result in a massive stimulation of an increased number of adrenalin receptors with result adrenalin over-stimulation, and the accompanying side effects of what is effectively an adrenalin over-dose.
Symptoms of such an extreme over-dose can include increased fatigue, joint or muscle pain, skin rashes, photosensitivity, irritability, paresthesia, dizziness, sleep disturbances, asthenia, muscle cramps, night sweats, hypertension, hypotension, headaches (especially migraines) and swollen glands. Also reported are heavy perspiration, metallic taste in mouth, chills, nausea, bloating, constipation or diarrhea, low grade fever, heart palpitations, tachycardia, facial palsy, tinnitus, mental confusion, uncoordinated movement, pruritus, bone pain, flu-like syndrome, conjunctivitis and throat swelling"
Overcoming the side-effects of Vitamin B12 supplementation
Given the potential seriousness of the vitamin B12 supplementation it is important that re-establishment of vitamin B12 sufficiency be under-taken with due care. Time must be given for the receptor numbers to either increase (for dopamine and serotonin) and for those for adrenalin to slowly decrease. Potentially this can takes weeks or even months of gradual increase in either methyl B12 or the co-factors such as vitamin B2, Iodine, Selenium and Molybdenum that are essential for maintenance of methyl Co(III)B12 activity. During this process it is important to be consistent in your approach, going too fast can lead to serious depression, and/or huge adrenalin over-dose reactions, with resultant side-effects.
MAO and inactivation of Adrenalin
The primary enzyme that inactivates adrenalin is the FAD-dependent enzyme, Mono-amineoxidase (MAO). MAO is a particularly long-lived enzyme, and so the turn-over rate of the enzyme is relatively long. FAD is incorporated covalemtnly into the enzyme at time of synthesis. This can pose a problem during the restoration of vitamin B2 activity as the activity of both MTHFR and MTRR can precede the restoration of MAO activity, with the result that the stimulation of adrenalin production can greatly enhance and prolong the adrenalin reaction due to the inability to inactivate it.
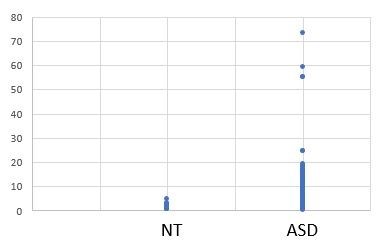
Overproduction of Dopamine and Nor adrenalin in vitamin B12 deficiency
The final step in production of adrenalin involves the methylation of the adrenalin precursor, nor-adrenalin, and in B12 deficiency (top panel), studies have shown (particularly in children with ASD) that this is greatly increased levels of dopamine and nor-adrenalin in serum and greatly increased levels of the break-down products HVA and VMA (Bottom panel). The high levels of these adrenalin precursors can mean that if methylation is restored there can be a massive increase in the local production of adrenalin.


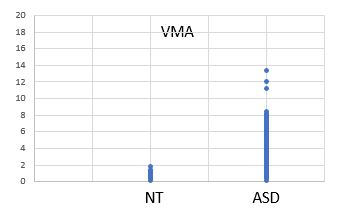
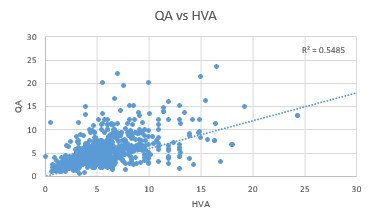
Overproduction of Serotonin in vitamin B12 Deficiency
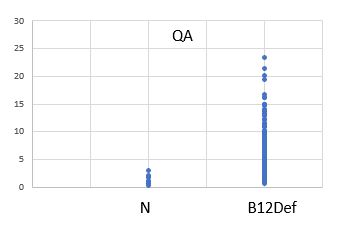
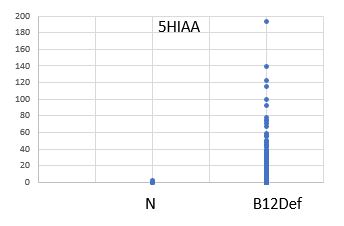
Production of Melatonin, requires Studies on children with ASD show greatly increased levels of the tryptophan break-down products QA and KA and greatly increased levels of the serotonin break-down product 5HIAA


SSRIs, vitamin B12 Deficiency and Depression
Many persons who have been prescribed anti-depressant drugs such as SSRIs and SNRIs have subsequently been found to either be overtly vitamin B12 deficient or have paradoxical B12 deficiency. Upon enquiry, we have yet to find one person whose doctor had checked for B12 deficiency by testing for levels of MMA, Homocysteine, or 5HIAA, or dopamine metabolites HVA/VMA or serotonin associated metabolites QA and KA. More particularly not one doctor could describe why vitamin B12 deficiency would result in elevated dopamine or serotonin, or who knew about paradoxical B12 deficiency (see https:/b12oils.com/paradoxical.htm ).
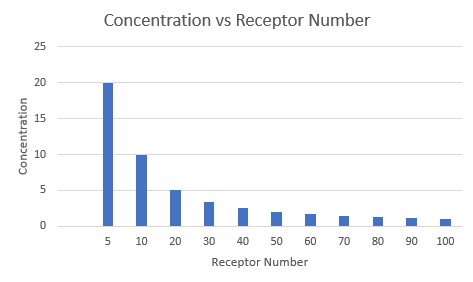
In the context of SSRIs one can see that as the concentration of the ligand changes, binding to variable numbers of receptors changes. Hence to have the same number of receptor hits, one can either increase the number of receptors or increase the concentration of the ligand/neurotransmitter. Hence, as more serotonin is made the number of receptors would decrease for the same stimulus.
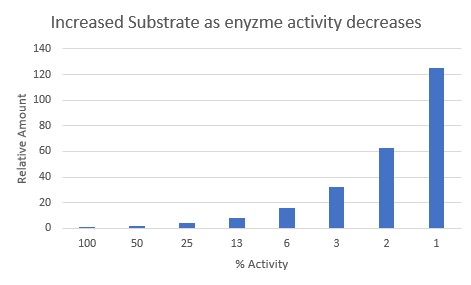
Many chemical reactions are governed by Le Chatelier's principle where in a reaction A + B <=> C + D, you can increase the product "D" by increasing A or B. In a similar fashion for an enzymatic reaction, such as the conversion of N-Acetyl Serotonin to melatonin, you can increase the rate of the reaction by increasing the uptake of the Tryptophan precursor and thereby increase the production of QA, KA, and 5HIAA, as seen above. Modeling of the reaction S => [C]*R => P for different rates of activity of the enzyme, shows dramatic needs for more substrate as the enzyme activity decreases.
Evidence that this is happening in vivo can be seen by the increased amounts of HVA and QA seen in functional vitamin B12 deficiency. Hence increases of 10 to 25 times in the concentrations of HVA and QA are common in vitamin B12 deficiency in ASD (and also in CFS), HVA will go up as the body tries to methylate nor-adrenalin to make adrenalin, whilst QA is a bypass pathway, which increases as the body tries to increase methylation of N-Acetyl Serotonin..
Side-effects of Vitamin B12 supplementation
Side effects of vitamin B12 supplementation can include symptoms of adrenalin overdose
A. increased fatigue, joint or muscle pain, skin rashes, photosensitivity, irritability, paresthesia, dizziness, sleep disturbances, asthenia, muscle cramps, night sweats, hypertension, hypotension, headaches (especially migraines) and swollen glands. Also reported are heavy perspiration, metallic taste in mouth, chills, nausea, bloating, constipation or diarrhea, low grade fever, heart palpitations, tachycardia, facial palsy, tinnitus, mental confusion, uncoordinated movement, pruritus, bone pain, flu-like syndrome, conjunctivitis and throat swelling"
B. worsened breathing trouble, sudden numbness or weakness on one side of the body, slurred speech, problems with vision or balance, or dangerously high blood pressure (severe headache, blurred vision, buzzing in your ears, anxiety, confusion, chest pain, shortness of breath, uneven heartbeats, seizure).
Side effects of Serotonin withdrawal include
Nausea, sweating, mood changes, particularly depression, anxiety, irritability, agitation, and dizziness, headache, confusion, lethargy and trouble sleeping. Reported side effects in children with autism have been reported as continous crying, screaming, not wanting anything or anyone to touch them, or being frightened if people come near them, classical symptoms of fear and anxiety. If such symptoms occur, increases in supplementation should be more gradual.
Over-production of serotonin, which may occur in persons who start to too rapidly lower serotonin levels and then yo-yo back by stopping the process, include
Shivering, confusion, high BP, dilated pupils, hallucinations, increased heart rate, headaches, good bumps, over active reflexes
Side effects of Dopamine withdrawal include
Anxiety, panic attacks, irritability, depression, hopelessness, lack of pleasure, fatigue, exhaustion, difficulty sleeping, pain and orthostatic hypotension, difficulty concentrating, cognitive changes, low motivation, funny tasting breath and low libido.
Copyright © 2018 B12 Oils. All Rights Reserved.
Reproduction in whole or in part in any form or medium without express written
permission is prohibited