
CFS, Methylation and Creatine
-
CFS/FM/ME can be a debilitating condition affecting around 3% of the population
-
The condition is generally misunderstood, however, symptoms are very similar to those seen with an absolute deficiency of vitamin B12
-
The condition is characterized by Paradoxical B12 deficiency
-
Studies on over 700 individuals have shown all have functional B2 deficiency
-
Functional B2 deficiency results in functional B12 deficiency.
-
Functional B2 deficiency leads to poor energy conversion from fat, sugar and protein, contributing to Constant Fatigue
-
The defining characteristic of the condition is reduced cycling of Methyl B12 and hence the under-production of creatine.
-
Over 40% of S-Adenosyl-Methionine (SAM) produced in the body is involved in the production of Creatine.
-
Lack of Creatine production results in prolonged lack of energy, with prolonged over-usage or underproduction eventually leading to the subject being chronically fatigued (CFS)
-
Reduced production of Creatine has been associated with many conditions including dementia, Parkinson's disease, Autism, Chronic Fatigue Syndrome.
-
Reduced methylation due to functional B12 deficiency results in depression, anxiety and poor sleep - common symptoms in CFS
-
Reduced methylation due to functional B12 deficiency, results in lower production of melatonin and poor maturation of the gut
Chronic Fatigue Syndrome (CFS) or Myalgic Encephalomyelitis (ME)
Chronic Fatigue Syndrome (CFS) or Myalgic Encephalomyalitis (ME) is an ill defined disease that is characterized by a post exercise tiredness or malaise. The condition usually lasts for more than six months and in affected individuals is very disabling. Symptoms include muscle soreness, inability to concentrate (brain fog), headaches and severe mental and physical fatigue. In addition these symptoms may be accompanied by sensitivity to light, sounds and smells, digestive disturbances, depression, painful and often slightly swollen lymph nodes, and it may also be accompanied by cardiac and respiratory problems.
Causes of CFS
A wide variety of immune, endocrine, cardiovascular and central nervous abnormalities have been reported in CFS. Among the causes suggested for CFS include damage to parts of the brain governing cognition, memory, mood, energy and perception, an altered stress response, an unbalanced immune system, a hidden chronic infection, excessive production of free radicals, reduced intracellular glutathione, abnormal sympathetic nervous system activity, cardiac dysfunction and others. Many CFS sufferers are found to have sub-normal levels of vitamin D in their serum. Several researchers believe that CFS is a mitochondrial disease in which excessive, uncontrolled production of nitric oxide damages proteins in the mitochondria, and particularly in the electron transport chain. Whilst the exact cause of CFS may vary, a major group of CFS sufferers have also been found to have one or more mutations in the enzymes responsible for methylation. In these individuals it would appear that whilst they were able to exist as relatively healthy individuals, often not knowing that they had methylation associated mutations, some initiating factor such as a prolonged infection, combined with low vitamin D levels resulted in gradual loss of their vitamin B12 supplies leading to the CFS symptomatology being apparent, and the subsequent discovery of their methylation status. A recent study by Russell-Jones (2022) has shown that every individual studied had a deficiency in functional vitamin B2. This deficiency appears to have been caused by an inadequate intake of Iodine, Selenium and/or Molybdenum, which in turn resulted in lower activation of vitamin B2. The functional vitamin B2 deficiency, in turn, resulted in gradual inactivation of vitamin B12. Individuals were found to be deficient in both Adenosyl and Methyl B12, yet serum vitamin B12 levels were normal or elevated.
Thus a situation of Paradoxical B12 deficiency was universal.Lyme Disease and CFS
A high proportion of those who contact us with CFS have had Lyme disease. It appears that the infective organism(s), that cause Lyme, such as the spirochete, Borrelia Burgdorferi, are either huge consumers of vitamin B2, or the inflammatory response the they generate depletes the body of vitamin B2, which in turn inactives vitamin B12, and it is the dual deficiencies that cause the CFS. In order to treat Lyme-CFS, one has to firstly control the organism, and then maker sure that the B2 and B12 are fixed (see the RnB protocol - https://b12oils.com/rnb.htm ).
Causes of Fatigue
The primary symptom of CFS/ME is fatigue, but few researchers appear to address this issue, however, resolving the fatigue would appear to be the primary aim of treatment. We have identified several known causes of fatigue and have outlined them in the cartoon below

Most would be familiar with the fatigue that one feels after over-exercising, when stores of muscle glycogen and creatine-phosphate are used up. Fatigue can also occur in vitamin B12 deficiency, due to the lack of production of the electron-transport vehicle CoQ10 (a methylation product) and due to lack of production of the ATP shuttle vector creatine. Fatigue is also common in hypothyroidism, in which lack of Iodine and/or Selenium results in lack of activation of vitamin B2, and that then affects the activation of vitamin B12, with functional vitamin B12 deficiency resulting. A feature of Chronic Fatigue is lack of functional B2 and functional B12, which can occur to prolonged infection, and/or constant over-training or over-work, the two most common causes of CFS/ME. The most likely cause of the fatigue is lack of production of creatine due to functional vitamin B12 deficiency (see below).
Vitamin B2 deficiency in CFS
Activation of vitamin B2 in the body requires all of Iodine, Selenium and/or Molybdenum, and at the top of this cascade is the requirement for an active thyroid. Our Data shows a very high level of hypothyroidism in women with CFS. This is in line with the observations that conditions such as fatigue, headaches, low body temperature, anxiety, panic attacks, PMS, hair loss, depression, low motivation, IBS, insomnia, decreased memory and concentration are all common symptoms in hypothyroidism.
Vitamin B12 deficiency in CFS
The main cause of CFS is functional vitamin B12 deficiency, however, vitamin B12 levels may be normal or higher than normal and present as Paradoxical B12 deficiency.
Synthesis of Creatine
Synthesis of creatine occurs in two steps
1. Conjugation of glycine, and arginine, via the enzyme, l-arginine:glycine amidinotransferase (AGAT), to produce guanidinoacetate acid (GAA),

2. Methylation of Guanidinoacetate by the enzyme Guanidinoacetate-N-Methyl transferase (GNMT, GAMT)
![]()
In many individuals a reduced production of the energy shuttle vector, CoQ10 is also found. CoQ10 production involves three methylation steps.
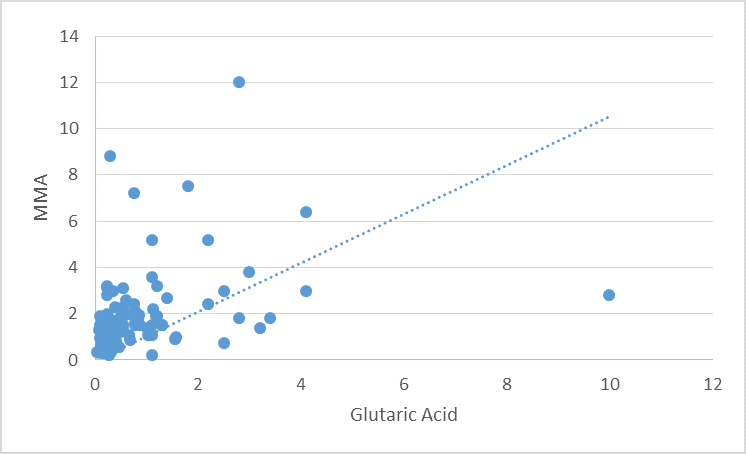
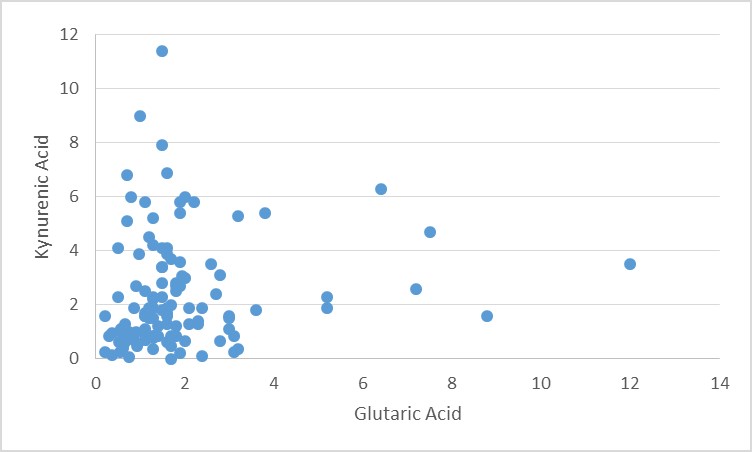
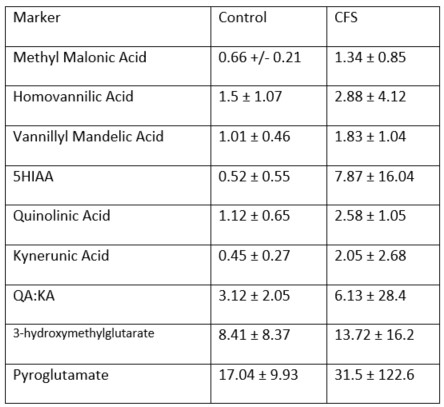
Functional B12 deficiency correlates with functional B2 deficiency.Functional vitamin B2 deficiency as determined by levels of glutaric acid in urine, correlated with both the classical marker of AdenosylB12 deficiency, as MMA gradually increased as glutaric acid levels increased, and with neurological markers of Methyl B12 deficiency.
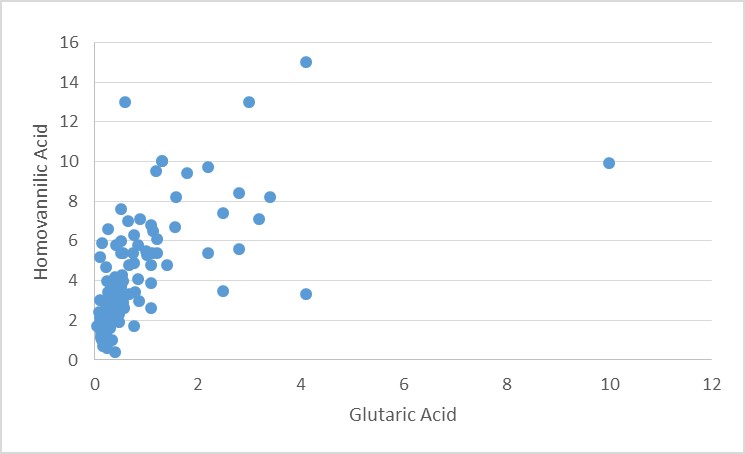
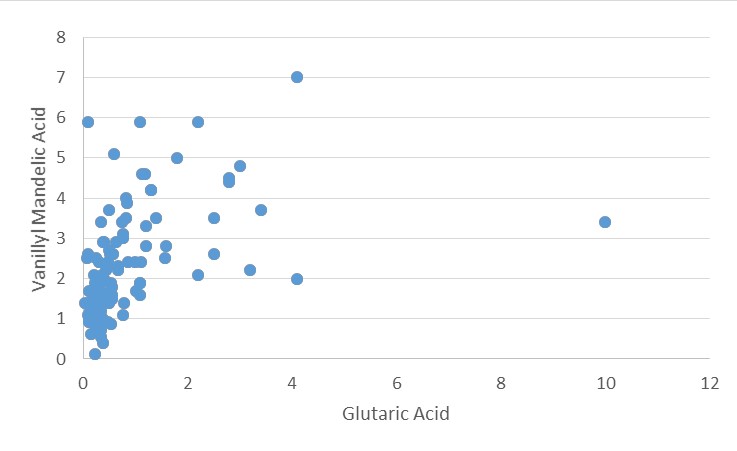
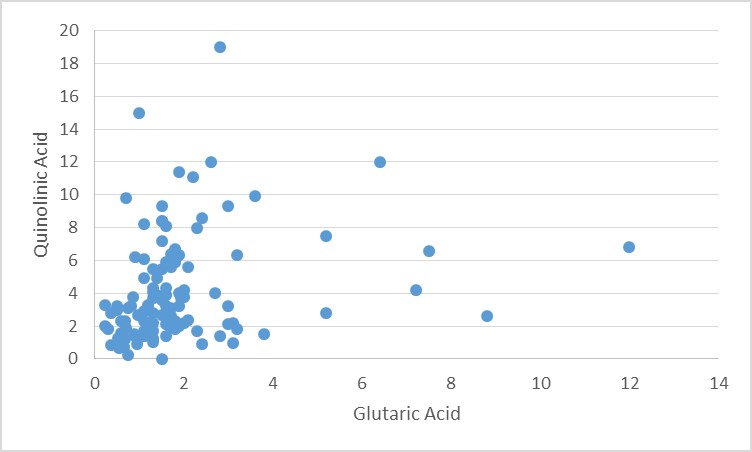
Similarly, other markers of Methyl B12 deficiency, Homovanillic acid, Vanillyl Mandelic acid, Quinolinic Acid and Kynurenic acid all increased as glutaric acid increased.
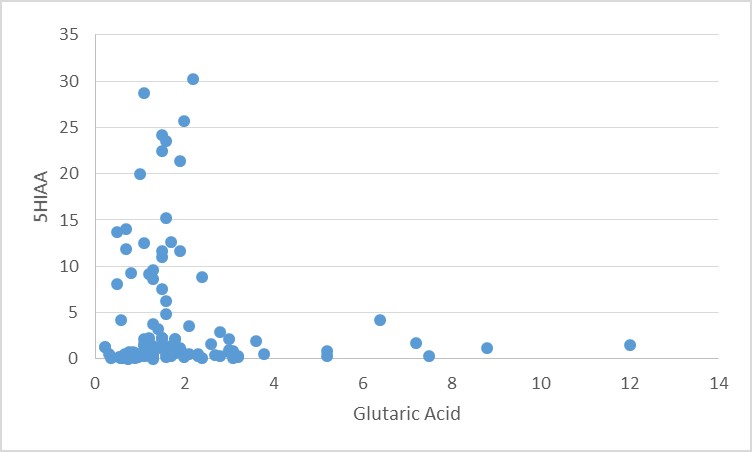
In contrast, initially levels of 5-hydoxyindole acetic acid increased as glutaric acid increased, however there was an inflection point at glutaric acid levels of 2 or above. This presumably reflects the requirement for functional vitamin B6 in the synthesis of serotonin. However, if functional B2 deficiency is great enough, then vitamin B6 activation (which requires FMN) will not occur.
Synthesis of melatonin requires methylation of N-AcetylSerotonin.

Synthetic pathway for Melatonin
Lack of vitamin B12 pushes the pathway to both degradation of serotonin, but also to the metabolic destruction of high levels of intracellular tryptophan with increased in KA and QA. In addition, the lack of B12 also results in reduced production of melatonin, contributing to poor gut health - often seen in CFS and also to poor sleep patterns, also characteristic of CFS.
Not only is there reduced production of melatonin and adrenalin in vitamin B12 deficiency, because of the requirement for methylation, there is also reduced production of CoQ10 and creatine, which are arguably the main contributing factors to the chronic fatigue seen in CFS, as these result in poor energy conversion, and gradual loss of stored muscle creatine.
The reduction in the rate of methylation also reduces the transfer of homocysteine into the sulphation cycle thereby resulting in lower production of Glutathione and increased production of pyroglutamate
The primary reason for the chronic fatigue seen in CFS is the reduced production of creatine, the energy transfer molecule within the cytoplasm of the cell. Given that over 40% of all methylation goes to the production of creatine, this would be consistent with this mechanism (see https://b12oils.com/creatine.htm). Mutations in the enzyme GAMT are associated with conditions such as autism. Deficiency in GAMT activity has been associated with conditions such as epilepsy, mental retardation and pyrimidal movement disorders (Ensenauer etal, 2004).
Iron Deficiency and CFS
Contributing to lower energy in CFS can be lower levels of iron, as this will reduce the amount of oxygen that can be used in oxidative phosphorylation, further it reduces the efficiency of the Electron Transport Chain (ETC). Of greater significance, though, is the uncoupling of the enzyme aconitase, the major enzyme involved in the metabolism of citrate in the citric acid. As ferritin levels drop below 70 ug/L, aconitase starts to reduce it ability to metabolize citric acid with the result that energy (as unmetabolized citrate) appears in urine. As ferritn drops to around 20 ug/L as much as 80-90% of citrate can be lost into urine. Optimal levels of iron, therefore should be with ferritin >70 ug/L, Haemoglobin >14.5 and Haematocrit >0.45.
Genetic Linkage
Recently it has been found that CFS may be related to defects in either folate metabolism and/or the methylation cycle, with a high incidence of sufferers have genetic mutations in the MTHFR, MTR, MTRR, MTS and/or SHMT genes. In addition many CFS individuals have genetically similar vitamin D receptor genes. It is possible that CFS sufferers have had these "inborn errors of metabolism" for much of their life, without experiencing any significant problem until some precipitating event such as stress or a chronic infection has triggered chemical changes inside the body thereby resulting in CFS.
Treatment of CFS
Many, many different treatments have been tried in an
attempt to cure CFS, with little success.
The RnB protocol has been found to be highly effective in reversing the symptoms of CFS
(RnB protocol)Creatine supplementation has also proven to have some success in some individuals (Allen, 2012).
Current Treatments of CFS
The majority of treatments as outlined by "Experts in the field" do not address
generation of creatine, rather are aimed at treating the symptoms. These
treatments are expensive (over $50K pa) and generally useless and include
Chelation therapy,
Graded exercise therapy guided by exercise physiologists
Cognitive behavioural therapy guided by clinical psychologists
Treatment of sleep disorders - by a sleep consultant
Treatment of depression, by a clinical psychiatrist, generally with the use of
SSRIs, or SNRIs or other addictive anti-depressants
References:
Regland B, Andersson M, Abrahamsson L, Bagby J, Dyrehag LE, Gottfries CG (1997). Increased concentrations of homocysteine in the cerebrospinal fluid in patients with fibromyalgia and chronic fatigue syndrome. Scand J Rheumatol. 26(4):301-7
Björkegren K. (1999) Vitamin B12, chronic fatigue and injection treatment. Lakartidningen. 96(50):5610.
Askmark H, Haggĺrd L, Nygren I, Punga AR. (2012) Vitamin D deficiency in patients with myasthenia gravis and improvement of fatigue after supplementation of vitamin D3: a pilot study. Eur J Neurol. 19(12):1554-60.
Yancey JR, Thomas SM. Chronic fatigue syndrome: diagnosis and treatment. Am Fam Physician. 2012 Oct 15;86(8):741-6. PMID: 23062157.
Bested AC, Marshall LM. Review of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: an evidence-based approach to diagnosis and management by clinicians. Rev Environ Health. 2015;30(4):223-49. doi: 10.1515/reveh-2015-0026. PMID: 26613325.
Rollnik JD. Das chronische Müdigkeitssyndrom – ein kritischer Diskurs [Chronic Fatigue Syndrome: A Critical Review]. Fortschr Neurol Psychiatr. 2017 Feb;85(2):79-85. German. doi: 10.1055/s-0042-121259. Epub 2017 Feb 24. PMID: 28235209.
Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, Komaroff A. The chronic fatigue syndrome: a comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann Intern Med. 1994 Dec 15;121(12):953-9. doi: 10.7326/0003-4819-121-12-199412150-00009. PMID: 7978722.
Blitshteyn S, Chopra P. Chronic Fatigue Syndrome: From Chronic Fatigue to More Specific Syndromes. Eur Neurol. 2018;80(1-2):73-77. doi: 10.1159/000493531. Epub 2018 Oct 4. PMID: 30286454.
Baklund IH, Dammen T, Moum TĹ, Kristiansen W, Duarte DS, Castro-Marrero J, Helland IB, Strand EB. Evaluating Routine Blood Tests According to Clinical Symptoms and Diagnostic Criteria in Individuals with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J Clin Med. 2021 Jul 14;10(14):3105. doi: 10.3390/jcm10143105. PMID: 34300271; PMCID: PMC8307418.
Kaslow JE, Rucker L, Onishi R. Liver extract-folic acid-cyanocobalamin vs placebo for chronic fatigue syndrome. Arch Intern Med. 1989 Nov;149(11):2501-3. PMID: 2684076.
Wiebe E. N of 1 trials. Managing patients with chronic fatigue syndrome: two case reports. Can Fam Physician. 1996 Nov;42:2214-7. PMID: 8939323; PMCID: PMC2146911.
Regland B, Forsmark S, Halaouate L, Matousek M, Peilot B, Zachrisson O, Gottfries CG. Response to vitamin B12 and folic acid in myalgic encephalomyelitis and fibromyalgia. PLoS One. 2015 Apr 22;10(4):e0124648. doi: 10.1371/journal.pone.0124648. PMID: 25902009; PMCID: PMC4406448.
Regland B. Vitamin B12/B9 – möjlig behandling vid mental trötthet [Vitamin B12/B9 – possible treatment for mental fatigue]. Lakartidningen. 2017 Jul 11;114:ERZ3. Swedish. PMID: 28696491.
Blankfield A. Kynurenine Pathway Pathologies: do Nicotinamide and Other Pathway Co-Factors have a Therapeutic Role in Reduction of Symptom Severity, Including Chronic Fatigue Syndrome (CFS) and Fibromyalgia (FM). Int J Tryptophan Res. 2013 Jul 21;6(Suppl 1):39-45. doi: 10.4137/IJTR.S11193. PMID: 23922501; PMCID: PMC3729338.
Blankfield A. A Brief Historic Overview of Clinical Disorders Associated with Tryptophan: The Relevance to Chronic Fatigue Syndrome (CFS) and Fibromyalgia (FM). Int J Tryptophan Res. 2012;5:27-32. doi: 10.4137/IJTR.S10085. Epub 2012 Sep 17. PMID: 23032646; PMCID: PMC3460668.
ABDULLA J, Torpy BDJ. Chronic Fatigue Syndrome. 2017 Apr 20. In: Feingold KR, Anawalt B, Boyce A, Chrousos G, de Herder WW, Dhatariya K, Dungan K, Hershman JM, Hofland J, Kalra S, Kaltsas G, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrčre B, Levy M, McGee EA, McLachlan R, Morley JE, New M, Purnell J, Sahay R, Singer F, Sperling MA, Stratakis CA, Trence DL, Wilson DP, editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000–. PMID: 25905324.
Rossi L, Nardecchia F, Pierigč F, Ventura R, Carducci C, Leuzzi V, Magnani M, Cabib S, Pascucci T. Intellectual Disability and Brain Creatine Deficit: Phenotyping of the Genetic Mouse Model for GAMT Deficiency. Genes (Basel). 2021 Aug 2;12(8):1201. doi: 10.3390/genes12081201. PMID: 34440375; PMCID: PMC8391
Modi BP, Khan HN, van der Lee R, Wasim M, Haaxma CA, Richmond PA, Drögemöller B, Shah S, Salomons G, van der Kloet FM, Vaz FM, van der Crabben SN, Ross CJ, Wasserman WW, van Karnebeek CDM, Awan FR. Adult GAMT deficiency: A literature review and report of two siblings. Mol Genet Metab Rep. 2021 Apr 26;27:100761. doi: 10.1016/j.ymgmr.2021.100761. PMID: 33996490; PMCID: PMC8093930.
Joncquel-Chevalier Curt M, Voicu PM, Fontaine M, Dessein AF, Porchet N, Mention-Mulliez K, Dobbelaere D, Soto-Ares G, Cheillan D, Vamecq J. Creatine biosynthesis and transport in health and disease. Biochimie. 2015 Dec;119:146-65. doi: 10.1016/j.biochi.2015.10.022. Epub 2015 Nov 2. PMID: 26542286.
Mercimek-Mahmutoglu S, Stoeckler-Ipsiroglu S, Adami A, Appleton R, Araújo HC, Duran M, Ensenauer R, Fernandez-Alvarez E, Garcia P, Grolik C, Item CB, Leuzzi V, Marquardt I, Mühl A, Saelke-Kellermann RA, Salomons GS, Schulze A, Surtees R, van der Knaap MS, Vasconcelos R, Verhoeven NM, Vilarinho L, Wilichowski E, Jakobs C. GAMT deficiency: features, treatment, and outcome in an inborn error of creatine synthesis. Neurology. 2006 Aug 8;67(3):480-4. doi: 10.1212/01.wnl.0000234852.43688.bf. Epub 2006 Jul 19. PMID: 16855203.
Gordon N. Guanidinoacetate methyltransferase deficiency (GAMT). Brain Dev. 2010 Feb;32(2):79-81. doi: 10.1016/j.braindev.2009.01.008. Epub 2009 Mar 16. PMID: 19289269.
Nasrallah F, Kraoua I, Joncquel-Chevalier Curt M, Bout MA, Taieb SH, Feki M, Khouja N, Briand G, Kaabachi N. Guanidinoacetate methyltransferase (GAMT) deficiency in two Tunisian siblings: clinical and biochemical features. Clin Lab. 2012;58(5-6):427-32. PMID: 22783571.
Pérez B, Medrano C, Ecay MJ, Ruiz-Sala P, Martínez-Pardo M, Ugarte M, Pérez-Cerdá C. A novel congenital disorder of glycosylation type without central nervous system involvement caused by mutations in the phosphoglucomutase 1 gene. J Inherit Metab Dis. 2013 May;36(3):535-42. doi: 10.1007/s10545-012-9525-7. Epub 2012 Sep 14. PMID: 22976764.
Sahlin K, Tonkonogi M, Söderlund K. Energy supply and muscle fatigue in humans. Acta Physiol Scand. 1998 Mar;162(3):261-6. doi: 10.1046/j.1365-201X.1998.0298f.x. PMID: 9578371.
Clark JB, Hayes DJ, Morgan-Hughes JA, Byrne E. Mitochondrial myopathies: disorders of the respiratory chain and oxidative phosphorylation. J Inherit Metab Dis. 1984;7 Suppl 1:62-8. doi: 10.1007/BF03047377. PMID: 6434847.
Sobreira C, Hirano M, Shanske S, Keller RK, Haller RG, Davidson E, Santorelli FM, Miranda AF, Bonilla E, Mojon DS, Barreira AA, King MP, DiMauro S. Mitochondrial encephalomyopathy with coenzyme Q10 deficiency. Neurology. 1997 May;48(5):1238-43. doi: 10.1212/wnl.48.5.1238. PMID: 9153450.
Kan, HE, Buse-Pot TE, Peco R, Isbrandt D, Heerschap A, de Haan A. Lower force and impaired performance during high-intensity electrical stimulation in skeletal muscle of GAMT-deficient knockout mice. Am J Physiol Cell Physiol. 2005 Jul;289(1):C113-9. doi: 10.1152/ajpcell.00040.2005. Epub 2005 Mar 2. PMID: 15743892.
Mercimek-Mahmutoglu S, Stoeckler-Ipsiroglu S, Adami A, Appleton R, Araújo HC, Duran M, Ensenauer R, Fernandez-Alvarez E, Garcia P, Grolik C, Item CB, Leuzzi V, Marquardt I, Mühl A, Saelke-Kellermann RA, Salomons GS, Schulze A, Surtees R, van der Knaap MS, Vasconcelos R, Verhoeven NM, Vilarinho L, Wilichowski E, Jakobs C. GAMT deficiency: features, treatment, and outcome in an inborn error of creatine synthesis. Neurology. 2006 Aug 8;67(3):480-4. doi: 10.1212/01.wnl.0000234852.43688.bf. Epub 2006 Jul 19. PMID: 16855203.
Strahler J, Fischer S, Nater UM, Ehlert U, Gaab J. Norepinephrine and epinephrine responses to physiological and pharmacological stimulation in chronic fatigue syndrome. Biol Psychol. 2013 Sep;94(1):160-6. doi: 10.1016/j.biopsycho.2013.06.002. Epub 2013 Jun 13. PMID: 23770415.
Morriss R. Insomnia in the chronic fatigue syndrome. BMJ. 1993 Jul 24;307(6898):264. doi: 10.1136/bmj.307.6898.264. PMID: 8369716; PMCID: PMC1678179.
Galvez-Sánchez CM, Duschek S, Reyes Del Paso GA. Psychological impact of fibromyalgia: current perspectives. Psychol Res Behav Manag. 2019 Feb 13;12:117-127. doi: 10.2147/PRBM.S178240. PMID: 30858740; PMCID: PMC6386210.
Welsch P, Üçeyler N, Klose P, Walitt B, Häuser W. Serotonin and noradrenaline reuptake inhibitors (SNRIs) for fibromyalgia. Cochrane Database Syst Rev. 2018 Feb 28;2(2):CD010292. doi: 10.1002/14651858.CD010292.pub2. PMID: 29489029; PMCID: PMC5846183.
Pejovic S, Natelson BH, Basta M, Fernandez-Mendoza J, Mahr F, Vgontzas AN. Chronic fatigue syndrome and fibromyalgia in diagnosed sleep disorders: a further test of the 'unitary' hypothesis. BMC Neurol. 2015 Apr 12;15:53. doi: 10.1186/s12883-015-0308-2. PMID: 25884538; PMCID: PMC4405866.
Campbell R, Vansteenkiste M, Delesie L, Tobback E, Mariman A, Vogelaers D, Mouratidis A. Reciprocal associations between daily need-based experiences, energy, and sleep in chronic fatigue syndrome. Health Psychol. 2018 Dec;37(12):1168-1178. doi: 10.1037/hea0000621. Epub 2018 Oct 15. PMID: 30321019.
Tobback E, Desmet O, Hanoulle I, Delesie L, Pevernagie D, Vogelaers D, Mariman A. Retrospective Analysis of Risk Factors for Periodic Limb Movements in a Large Cohort of Insomnia and Chronic Fatigue Patients. Pharmacopsychiatry. 2020 Mar;53(2):71-77. doi: 10.1055/a-0991-0498. Epub 2019 Aug 27. PMID: 31454848.
Wright A, Fisher PL, Baker N, O'Rourke L, Cherry MG. Perfectionism, depression and anxiety in chronic fatigue syndrome: A systematic review. J Psychosom Res. 2021 Jan;140:110322. doi: 10.1016/j.jpsychores.2020.110322. Epub 2020 Dec 1. PMID: 33278659.
Loades ME, Read R, Smith L, Higson-Sweeney NT, Laffan A, Stallard P, Kessler D, Crawley E. How common are depression and anxiety in adolescents with chronic fatigue syndrome (CFS) and how should we screen for these mental health co-morbidities? A clinical cohort study. Eur Child Adolesc Psychiatry. 2021 Nov;30(11):1733-1743. doi: 10.1007/s00787-020-01646-w. Epub 2020 Sep 22. PMID: 32964335; PMCID: PMC8558286.
Groven N, Reitan SK, Fors EA, Guzey IC. Kynurenine metabolites and ratios differ between Chronic Fatigue Syndrome, Fibromyalgia, and healthy controls. Psychoneuroendocrinology. 2021 Sep;131:105287. doi: 10.1016/j.psyneuen.2021.105287. Epub 2021 May 27. PMID: 34090138.
Daniels J, Brigden A, Kacorova A. Anxiety and depression in chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME): Examining the incidence of health anxiety in CFS/ME. Psychol Psychother. 2017 Sep;90(3):502-509. doi: 10.1111/papt.12118. Epub 2017 Feb 28. PMID: 28244209.
Stoll SVE, Crawley E, Richards V, Lal N, Brigden A, Loades ME. What treatments work for anxiety in children with chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME)? Systematic review. BMJ Open. 2017 Sep 5;7(9):e015481. doi: 10.1136/bmjopen-2016-015481. PMID: 28877941; PMCID: PMC5588976.
Allen PJ. Creatine metabolism and psychiatric disorders: Does creatine supplementation have therapeutic value? Neurosci Biobehav Rev. 2012 May;36(5):1442-62. doi: 10.1016/j.neubiorev.2012.03.005. Epub 2012 Mar 24. PMID: 22465051; PMCID: PMC3340488.
Ensenauer R, Thiel T, Schwab KO, Tacke U, Stöckler-Ipsiroglu S, Schulze A, Hennig J, Lehnert W. Guanidinoacetate methyltransferase deficiency: differences of creatine uptake in human brain and muscle. Mol Genet Metab. 2004 Jul;82(3):208-13. doi: 10.1016/j.ymgme.2004.04.005. PMID: 15234333.
Russell-Jones, GJ 2022 Functional vitamin B12 deficiency in CFS. Int J. Psychiatry 27 Jul 2022 PDF
Russell-Jones, GJ 2022 Paradoxical vitamin B12 deficiency PDF
https://ammes.org/2022/08/20/functional-vitamin-b12-deficiency-in-chronic-fatigue-syndrome/
Copyright © 2021 B12 Oils. All Rights Reserved.
Reproduction in whole or in part in any form or medium without express written
permission is prohibited